Hot topic
PENG Research and Audit Grant
Management of Ileostomy Patients in a University Teaching Hospital
Melanie Baker, Senior Specialist Dietitian
As a Nutrition Support Team Dietitian I support patients with intestinal failure. This involves those with classical short bowel syndrome, requiring parenteral nutrition but also those whom can maintain their nutritional status orally but need parenteral fluid and electrolyte support. A cohort of these patients are referred to our team after multiple re-admissions to hospital with complications related to dehydration. This has led me to consider and evaluate our own local practice in relation to the management of these patients. Here I will provide a summary and also show how an application to the PENG research and audit grant has helped collect important evidence.
I applied for a PENG research and audit grant in 2015 and was successfully awarded £4,100 to undertake a retrospective audit. The PENG grant was a great opportunity of undertake some audit work in dedicated, funded time. Ultimately, I hope to undertake a prospective research project investigating dietetic support for this group of patients. Completing a robust, peer reviewed application at this early stage is really useful experience when considering future applications for funding. Grant awarding bodies look for evidence of publications and attainment of even small amounts of funding, so it is also a good addition to my CV.
Current evidence base
Formation of a small bowel stoma, as either a temporary or permanent measure is a common procedure in those with cancer, inflammatory bowel disease or in the surgical management of complications, such as perforation. It is estimated that approximately 45,000 people have an ileostomy and 21,000 stoma operations (colostomies and ileostomies) are performed annually in the UK (Colostomy Association, 2014).
Complications related to excessive stoma output have led to the development of evidence based guidelines, but historically these have related to those with short bowel syndrome (Nightingale & Woodward, 2006). Issues related to high stoma output and dehydration may occur outside of the short bowel population. Our own local published data showed that 50% of those presenting with a high output stoma during their admission after stoma formation had no known cause identified (Baker et al, 2011). There is also emerging evidence from cohort studies suggesting readmission rates due to dehydration in the region of 20-40% in the early months after surgery (Glasgow et al, 2014; Hayden et al, 2013).
There is a lack of evidence regarding nutritional status in the months after ileostomy formation. Three small studies have shown those with malnutrition are more likely to have complications (Bong-Hyeon et al, 2013; Kim et al, 2012; Altayeb et al, 2013). Mohil et al, (2012) reported > 10% weight loss in 43% of patients six weeks after emergency ileostomy, with significant reductions seen in tricep skinfold thickness and mid upper arm muscle circumference.
Oral intake from diet and fluids may have a role to play in the management of complications such as malnutrition and dehydration but there is a paucity of evidence to date in this clinical group. Published evidence for dietary changes in those with a stoma is based mainly on cross sectional study designs in heterogeneous populations, a long time after surgery (Bingham et al, 1986; Cohen et al, 2013). No study has prospectively assessed nutritional needs in the early months after stoma formation in terms of nutritional assessment and change in diet.
Evaluating local practice
Locally we have management guidelines for those with a high output stoma (HOS) but there is a lack of consensus to what constituents a HOS and we were concerned that not all effected patients were being appropriately identified and managed.
A retrospective audit was designed to assess:
- Prevalence of high output stomas (during the admission after stoma formation & re-admission in the first six months after stoma formation). Our current guidelines define a HOS as those with an outcome of >2000 ml daily for more than three days or <200 cm small bowel remaining or ongoing hydration or electrolyte abnormalities even if stoma volume is 1000 – 2000 ml daily.
- Use of current management guidelines (in terms of medication, fluid regimens use).
- Appropriate use of nutritional screening using ‘Malnutrition Universal Screening Tool’ (‘MUST’) with onward referral as indicated.
Key audit results
- 107 patients were identified from procedural coding data, validated against colorectal cancer audit information and nutrition team case notes. Medical notes were available in 93 (87%) cases. We excluded <18 years of age, those having refashioning of an existing stoma or those who died within one week of surgery .
- 16 (17%) had a documented high output stoma (HOS) during their index admission after surgery, although in two of these stoma outputs were never recorded above 1500ml/d. The use of anti-diarrhoeal, anti-secretory medication and appropriate oral fluid regimens (hypotonic fluid restrictions and use of electrolyte replacement solutions) was poor and there was evidence that local guidance were not fully adhered too.
- 12 (13%) patients were readmitted in the six months after stoma formation for complications related to stoma function (electrolyte abnormalities with hyponatraemia seen in all patients). In total there were 27 admissions in 12 patients although a HOS was only documented in 4/27 (15%). Again, use of HOS guidelines was patchy.
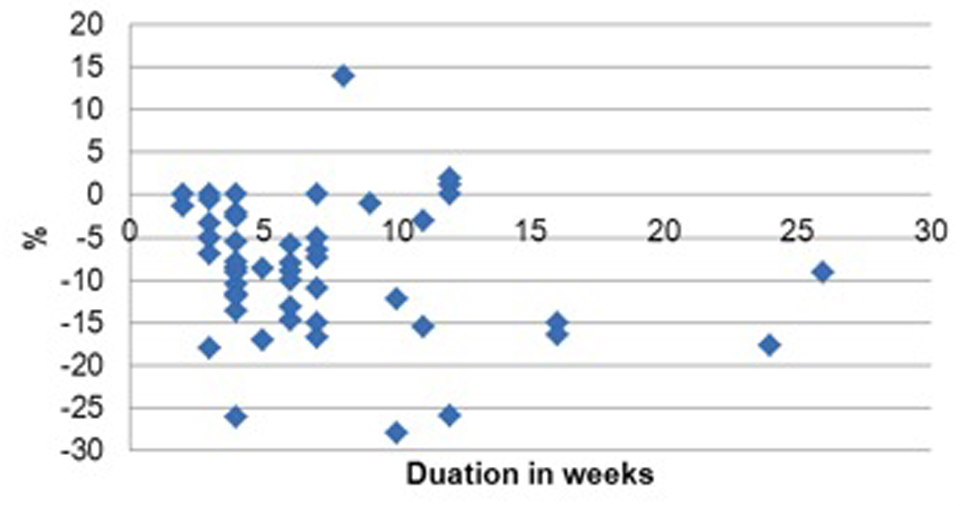
- In terms of nutritional screening, on admission 79/93 (85%) patients had evidence of a completed MUST although in 10% of these it was incorrect as recent weight loss had not been appropriately considered. In 52 (56%) there was evidence of post-operative weight measurement performed an average of 7 weeks (range 2 – 26 weeks) after operation. 31% had lost >10% weight compared with pre-surgery values (Figure A).
Figure A: Weight change post ileostomy
Implications for practice
The audit has demonstrated the need for training and education around management of HOS especially in non surgical clinical areas where patients may be re-admitted. Further evidence will now be collected to demonstrate that appropriately follow-up can prevent re-admission to obtain funding for a dedicated outpatient clinic.
Weight loss has been shown to occur in the months after surgery but further information is required to fully assess the implications of this (in terms of change in fat and lean body mass stores, effect on other outcomes such as quality of life and recovery and whether those with an ileostomy are at increased risk compared to other types of colorectal surgery). Initially the use of nutritional screening and appropriate onward dietetic referral at outpatient follow-up needs to be discussed and agreed locally.
PENG is keen to support Dietitians wanted to gain more experience in clinically relevant nutritional support research and audit. This was the subject of a well-attended research symposium in November 2015. Further details and presentations are available on the PENG website. Details can also be found on how to apply for a PENG grant.
References: Altayeb J, et al (2013). Reduction in body weight predicting metabolic complication of newly formed ileostomy. International Journal of Surgery; 589: 685. • Baker M L, Williams R N & Nightingale JMD (2011). Causes and management of a high-output stoma, Colorectal Diseases; 13(2): 191-7. • Bingham S, et al (2009). Diet and health of people with an ileostomy. British Journal of Nutrition; 47: 399-406. • Bong-Hyeon K, et al (2013). The nutritional impact of diverting stoma-related complications in elderly rectal cancer patients, International Journal of Colorectal Disease; 28: 1393-1400. • Colostomy Association. Accessed online: www.colostomyassociation.org.uk/ (Jan 2015). • Cohen AB, et al (2013). Dietary patterns and self-reported associations of diet with symptoms of inflammatory bowel disease. Digestive Diseases and Sciences; 581322–1328. • Glasgow MA, Shields K, Vogel RI (2014). Post-operative readmissions following ileostomy formation among patients with a gynecologic malignancy. Gynecologic Oncology; 134(3): 561-565. • Hayden DM, et al (2013). Hospital Readmission for Fluid and Electrolyte Abnormalities Following Ileostomy Construction: Preventable or Unpredictable? Journal of Gastrointestinal Surgery; 17: 298-303. • Hyun-Jung K, et al (2012). Comparison of nutrition status and nutrient intake for pre-and post-operative one month according to the type of operation for colorectal cancer Clinical Nutrition; 7(1): 76-77. • Kim MS et al (2012). The influence of Nutritional Assessment on the outcome of Ostomy Takedown Journal of the Korean Society of Coloproctology; 28(3): 145-151. • Mohil R S, et al (2012). Challenges of managing emergency ileostomy: Nutrition – A neglected aspect ISRN Emergency Medicine. Accessed online: http://www.hindawi.com/journals/isrn/2012/968023/ (March 2016). • Nightingale J, Woodward J (2006). Guidelines for Management of Patients with a short bowel. Gut, 55(6): 1-12.