
Hot topics
ESICM Lives 2015 28th Annual Conference
City Cube, Berlin, 3rd – 7th October 2015
Eileen O’Neill, PENG Committee Member
I was fortunate enough to attend the European Society of Intensive Care Medicine conference this year from the 5th-7th October. The pre-congress started on the 3rd October, running PG courses until the 4th when the opening ceremony took place. The main scientific programme ran 5th-7th October. The conference format included abstract presentations, oral presentations, poster corners, hot topics sessions and industry sponsored sessions, amongst others.
The key nutrition-related sessions focused on hypocaloric feeding, nutritional monitoring, including the importance of protein, and dysphagia. Throughout the conference there appeared to be an increased awareness of refeeding syndrome and discussions regarding continuous blood glucose monitoring, which I have not commented on below.
Hypocaloric feeding during the acute phase of critical illness
One of the thematic sessions focused on hypocaloric feeding, discussing what this involves, whether this is better for our patients and hypocaloric feeding in those with ‘chronic’ critical illness. Olav Rooyackers from Sweden introduced the topic by discussing the definition of hypocaloric feeding, whether this is low calorie/target protein, low calorie/low protein or whether this is an overall nutrient restriction. He also discussed whether energy expenditure is the same as energy need, i.e. if using direct or indirect calorimetry this equates to calorie targets, or not.
Michael Casear from Belgium suggested that hypocaloric feeding in the acute phase of critical illness results in a similar 90 day mortality outcome, compared to full feeding. Hypocaloric feeding has been defined as 40-60% of target energy needs and full feeding 70-100%. He did highlight that frequently patients at high risk of malnutrition are omitted from these studies and the definition of hypocaloric versus control varies from study to study.
Anne Berit Guttormsen from Norway highlighted that ~40% of ICU patients lose >10kg during their stay, on average patients receive 61% of their target calorie needs, are fed after around 38 hours and that 74% of patients are fed less than 80% of their target needs. She conveyed to the group the importance of assessing individual patients and whether hypocaloric feeding is appropriate for them. She suggested that those with ‘chronic’ critical illness, tracheostomies or were on ICU longer than around a week were perhaps not suitable for hypocaloric feeding. The patients at highest risk of malnutrition benefit from early feeding and hypocaloric feeding can be deleterious for these patients. If the patient is in the rehab phase the emphasis should be on maximising calorie and protein intake with the suggestion of increased energy expenditure up to 190% and aiming for 1.5-2g/kg protein today.

Nutritional monitoring in ICU
Peter Wejis from Amsterdam introduced the topic stating that ICU patients experience approximately 800 g protein loss in the initial 5 days of their stay, and patients experience approximately 20% loss of muscle mass after 10 days in hospital. An increased risk of mortality is shown in the low muscle group.
He summarised the research in this area, some of which also discussed permissive underfeeding. It has been found that permissive underfeeding of ~80% energy requirements in control group, ~50% requirements in permissive underfeeding group, and meeting ~80% of protein requirements for both groups, showed no difference in outcome. The population group was, however, young and those with BMI ~30kg/m2, not deemed at risk of malnutrition. Suggestions of protein requirements range from 1.2-2.5 g/kg/day, depending on clinical condition and phase of illness. Meeting >80% of protein requirements resulted in greater survival at 6 months.
Jan Wernerman from Stockholm discussed nutritional monitoring in the ICU, highlighting the importance of identifying patients at risk of malnutrition and limitations of using screening tools on an ICU. He described an increased risk of infection associated with increased energy deficit and agreed that considering nutritional status, comorbidities and acute disease are important when deciding what to feed patients. He also advised to consider whether patients are in the acute phase, in stable multi organ failure or rehab phase. He suggested avoiding undernutrition, and monitoring the balance of kcal and protein provided and that long stay patients benefit most from adequate feeding.
Dysphagia in mechanically ventilated ICU patients
Martin Dunser from Austria opened the session by discussing the incidence and outcomes of dysphagia on the ICU. He explained this was commonly under recognised, with the incidence of dysphagia ranging from 3-62%, up to 91% in those with critical illness polyneuropathy on a neuro ICU.
Swallow tests are commonly being performed by ICU nurses using 5-90ml of water, with videofluroscopy (VF) and fibre optic endoscopic evaluation of swallowing (FEES) becoming more common on ICU. Patients with dysphagia have been shown to have an increased risk of mortality, pneumonia and reintubation, resulting in increased cost, length of stay and malnutrition. Preventing further aspiration using dietary changes, nil by mouth and postural changes if required is common. Treatment included involving the multi-disciplinary team (MDT) such as speech and language therapy (SALT) in swallow/speech training and physiotherapy for muscle strength.  The dysphagia seen in critical illness polyneuropathy is generally reversible with 95% recovery after 4 weeks.
The dysphagia seen in critical illness polyneuropathy is generally reversible with 95% recovery after 4 weeks.
Rainer Dziewas from Germany discussed FEES in ICU to guide airway management decisions. A screening pathway was recommended using water and observing for cough, voice change, stridor, reduced saturations. This does, however, have a poor sensitivity and predictivity, and does not detect silent aspiration with a FEES recommended in high risk patients.
Didier Payen from France discussed swallowing disorders as a predictor of unsuccessful extubation. The ability to cough and expectorate may be linked with swallow dysfunction and the risk of unsuccessful extubation in these patients was around 15%.
The British Specialist Nutrition Association (BSNA) Survey Provides Insights into the Healthcare Professional’s Perception of Current Guidance and Training
The understanding and use of parenteral nutrition (PN) varies considerably amongst healthcare professionals (HCPs) and between Trusts across the UK. Recent studies such as NCEPOD1 and the CALORIES trial2 have provided insight into PN practices in the UK and its safety as an effective route for delivery of early nutrition support.
In order to better understand the current practices for providing PN and to gain an insight into the view of PN amongst HCPs in the UK, the British Specialist Nutrition Association (BSNA), which represents manufacturers of PN, conducted an online survey amongst 204 HCPs. Responses to the questionnaire were gathered from dietitians, pharmacists, nurses, gastroenterologists, intensive care specialists and oncologists.
The results reveal that the perception of PN could be improved by providing HCPs with more training and clearer guidance.
Clear guidance for healthcare professionals regarding the appropriate use of PN
Clinical guidelines (CGs), such as NICE CG323 and the European Society for Clinical Nutrition and Metabolism (ESPEN),4 aim to help HCPs correctly identify people in hospital and in the community who need nutrition support, and enable them to choose and deliver the most appropriate nutrition support at the most appropriate time. According to the survey results, the majority of HCPs were familiar with NICE CG323 (73%) and ESPEN guidelines on PN4 (73%). However, despite familiarity with NICE CG32,3 the findings of our survey highlighted a disparity between the advice given and its interpretation. Whilst 94% of HCPS agreed that ‘PN should be considered for all patients with a non-functioning, inaccessible or perforated gastrointestinal tract’, only 60% agreed that ‘PN should be considered for all patients with malnutrition and with inadequate/unsafe oral/enteral nutritional intake’ (figure 1); both statements are from NICE CG32.3 The survey also highlights the fact that without a clear consensus, treatment of PN may vary across care settings as 45% of HCPs disagreed with the NICE CG32 statement that ‘there is no minimum length of time for the duration in which PN can be given’.3
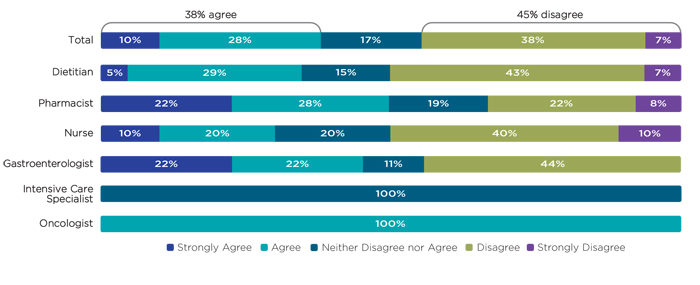 Figure 1 shows HCPs’ (n=204) levels of agreement when asked whether PN should be considered for all patients with malnutrition and with inadequate/ unsafe oral/ enteral nutrition intake, categorised by profession.
Figure 1 shows HCPs’ (n=204) levels of agreement when asked whether PN should be considered for all patients with malnutrition and with inadequate/ unsafe oral/ enteral nutrition intake, categorised by profession.
Improve the confidence of healthcare professionals to manage patients receiving PN at home
The survey findings demonstrate that the majority of respondents reported relatively high levels of confidence in the assessment, management and monitoring of patients receiving PN: 92% of HCPs reported feeling confident at assessing whether PN is appropriate for a patient; 91% of HCPS reported feeling confident at adjusting PN prescriptions to meet changing patient needs; and 96% of HCPs reported feeling confident at monitoring fluid balance and biochemical markers. However, results showed low levels of confidence among HCPs for training a patient to self-administer or preparing for discharge on to home PN – of the 57 HCPs (28% of total respondents) who considered the question applicable to them, only 16% reported feeling confident at training a patient to manage and self-administer PN, the majority of which were nurses. PN is used in community settings allowing patients to receive life-saving nutrition support in the comfort of their own home. These results indicate a need for further training to appropriate HCPs on preparing patients for independent use of PN.
Ensure that the appropriate healthcare professionals are adequately supported to prescribe PN
As PN is provided to patients on prescription, a PN regime can be recommended for a patient by a member of the nutrition support team, such as a dietitian or nurse, but the prescription must then be signed by an appropriate practitioner. At present this includes doctors and certain pharmacists. However, it was evident from qualitative feedback on the management of PN that participants support increasing the control dietitians have – as they are uniquely qualified to assess and manage a patient’s nutritional requirements – over prescribing PN by allowing them to become independent prescribers.
Consistent competency based nutrition training across all healthcare disciplines
The availability of PN training for HCPs differs between Trusts. The survey highlighted that in some cases training was done on the wards, and in other cases HCPs reported receiving training from external bodies, such as the British Pharmaceutical Nutrition Group (BPNG), or through the provision of Trust guidelines. A fifth of HCPs reported that their Trust didn’t provide any guidance or training on PN, a fifth also said that their Trust did not have a nutrition support team. There is a clear desire amongst HCPs for more formal, competency based, training at Trust level, in order to improve the way PN is prescribed and managed. A dietitian who responded to the survey said “more training that is suitable” whilst a gastroenterologist suggested “more trained and interested healthcare professionals involved”. Online training is the preferred mode of delivery however, practical courses and more detailed guidance were also popular suggestions of training tools.
Conclusion
The BSNA PN online survey provides an initial insight into HCPs views on PN and its use in the UK. The findings will hopefully lead to an increased awareness of the changes needed to improve the current use of PN in terms of patient care and training amongst HCPs. In order to achieve this, clearer guidance for HCPs on the appropriate use of PN needs to be provided and adequate support needs to be given to dietitians to enable them to prescribe PN. Finally, it is important that across all Trusts, the confidence of HCPs to educate home PN patients to manage their use of PN is improved. This will involve a concerted effort from industry and relevant HCP bodies
To access the full presentation of findings from the BSNA PN survey please click on the following link.
References: 1. Mason DG, et al (2010). A Mixed Bag. An enquiry into the care of hospital patients receiving parenteral nutrition. National Confidential Enquiry into Patient Outcome and Death (NCEPOD). Accessed online: www.ncepod.org.uk/2010report1/downloads/ PN_report.pdf (Sept 2015). 2. Harvey SE, et al (2014). Trial of the route of early nutritional support in critically ill adults. New England Journal of Medicine; 371 (18): 1673-1684. 3. NICE (2006). Nutrition support in adults: Oral nutrition support, enteral tube feeding and parenteral nutrition. NICE guidelines [CG32]. 4. Braga M, et al (2009). ESPEN guidelines on parenteral nutrition: surgery. Clinical nutrition; 28 (4): 378-386.